
What is Allergic Rhinitis?
Rhinitis refers to inflammation of the nasal passages which results in symptoms such as sneezing, nasal congestion and obstruction. Rhinitis which is caused by an allergic trigger is known as Allergic Rhinitis. This accounts for about 75% of rhinitis cases while the remaining 25% are termed non-allergic rhinitis.
Allergic Rhinitis may be medically classified as either intermittent or persistent. Allergic Rhinitis is classified as persistent if it is present for more than 4 days per week for more 4 consecutive weeks. The medical severity is then based on whether it impacts school, work, sleep, or sports.
Perennial Allergic Rhinitis occurs throughout the year and is most often caused by house dust mite and animal dander. Seasonal Allergic Rhinitis is known as Hay Fever and is caused by an allergy to pollen.
Causes of Allergic Rhinitis
The most common causes of Allergic Rhinitis are airborne allergens such as:
- Pollen
- House dust mite
- Mould
- Animal dander (cat, dog, horse, feathers etc)
Prevalence of Allergic Rhinitis
Allergic Rhinitis is a common condition with a global impact. It is estimated that allergic rhinitis affects at least 400 million people worldwide and that the prevalence in Europe is between 17 and 29%. In Ireland, we are likely to have a prevalence of about 26% in line with UK studies.
Pathophysiology of Allergic Rhinitis
Allergic Rhinitis occurs when the immune system misidentifies a specific airborne allergen as a threat and directs an inflammatory response against it. The immune system generates specific memory against the specific allergen so that any future exposure triggers an Immunoglobulin E (IgE) mediated immune response characterised by the release of histamine, leukotrienes, prostaglandins, kinins and other chemical mediators.
When the nasal passages are examined endoscopically in those who suffer from allergic rhinitis the findings often include bulky oedematous nasal turbinates with visibly increased mucus production. In chronic allergic rhinitis, the nasal mucosa can lose its smooth appearance and become pale and pitted. In some cases nasal polyps may develop and further aggravate the symptoms.
Genetic Predisposition to Allergic Rhinitis
The development of Allergic Rhinitis appears to be the consequence of environmental exposures in those with a genetic vulnerability. Indeed, genetic predisposition or atopy accounts for at least 50% of AR cases and genetic studies have demonstrated that multiple susceptible genetic loci can contribute to Allergic Rhinitis alone.
The Economic Impact of Allergic Rhinitis
The economic impact of Allergic Rhinitis is striking. The European Union recently estimated that the indirect cost of undertreated allergic rhinitis on work productivity is €30 - €50 billion per year.
What is non-allergic rhinitis?
Rhinitis that occurs without a known allergic trigger is called non-allergic rhinitis. This accounts for about 25% of rhinitis cases. Non-allergic rhinitis can be caused by structural nasal problems such septal deviation and nasal polyps but also through exposure to environmental pollution, chlorinated pools and even fragrances. Hormonal changes that occur during puberty, pregnancy and menopause can also act as a trigger.
In some cases, dysregulation of the autonomic nervous system characterised by increased parasympathic activity and reduced sympathetic activity is the culprit. This results in increased vascular permeability, mucosal swelling and increased mucus production.
Hay Fever (Seasonal Allergic Rhinitis)
Hay Fever affects people who are allergic to Grass, Tree or Plant Pollen. In addition to nasal and sinus symptoms, hay fever can also affect the eyes, lungs and skin. Most sufferers are allergic to grass pollen alone but 25% of those with grass pollen allergy also suffer from tree pollen allergy. It is also relatively common to have an allergy to tree or plant pollen without having an allergy to grass pollen.
When is Hay Fever Season in Ireland?
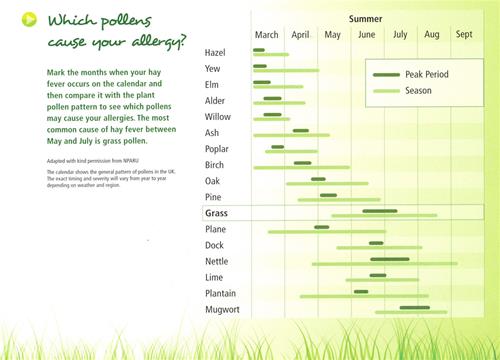 The Hay Fever season in Ireland occurs mainly in spring and summer but it can last until autumn. It begins with the release of Tree Pollen in early March until late May. This is followed by the Grass Pollen season which occurs from May until September. For those with the extra burden of mould spore allergy the hay fever season can drag on through the autumn months.
The Hay Fever season in Ireland occurs mainly in spring and summer but it can last until autumn. It begins with the release of Tree Pollen in early March until late May. This is followed by the Grass Pollen season which occurs from May until September. For those with the extra burden of mould spore allergy the hay fever season can drag on through the autumn months.
Impacts of Hay Fever
In addition to missed workdays in adults, allergic rhinitis can have a significant impact on a child’s education. Missed or unproductive days at school are common. This can become particularly significant as hay fever season coincides with exam time. A UK study of teenagers found that there was a reduction in exam performance for those with hay fever compared with other times of the year. This is most relevant for Leaving Certificate students and those in University.
What are the Symptoms of Hay Fever?
- Runny nose, sneezing and nasal congestion
- Sinus pressure and pain.
- Itchy red eyes +/- puffiness around the eyes.
- Cough or wheezing.
- Ears popping +/- hearing impairment.
- Reduced sense of taste and smell.
- Itchiness of the roof of the mouth.
- Feeling of fatigue or lethargy.
Hay Fever Symptoms explained
- Blocked nose: This is caused by inflammatory swelling of the nasal mucosa and nasal turbinates.
- Sneezing: The nasal lining becomes irritable and peppered with tiny blister-like swellings.
- Runny nose: The irritated nasal lining produces excessive mucus.
- Sinus pain: The passages from the nose to the sinuses become swollen and blocked, leading to increased pressure within the sinuses. This manifests as discomfort and pain in the forehead (frontal sinuses) and cheek bones (maxillary sinuses).
- Reduced sense of smell and taste: In severe cases, mucosal swelling within the nasal cavity compresses the olfactory nerve endings in the upper part of the nose. The sense of smell is affected and may be followed by a diminished sense of taste.
- Itchiness of the roof of the mouth: The roof of the mouth lies directly below the base of the maxillary sinuses and may become irritated by the adjacent sinus inflammation.
- Reduced hearing and ear popping: Swelling of the nasopharynx may impair the normal functioning of the eustachian tube.
- Cough, wheeze or shortness of breath: Inflammation of the nose and sinuses increases the reactivity and irritability of the lower respiratory tract. This may worsen existing asthma or trigger asthmatic symptoms in non-asthmatics.
- Itchy red eyes: Pollen irritates the eyes and the inner surface of the eye lids may distort with the telltale ‘cobble-stone’ appearance of allergic conjunctivitis.
- Fatigue: These symptoms can leave hay fever sufferers feeling exhausted and drained.
How is Hay Fever diagnosed?
The diagnosis of Hay Fever is usually based on the clinical symptoms and a medical examination. It is important to ensure that your nose, eye and chest symptoms are indeed caused by pollen allergy and not by another medical condition. At Allergy Ireland, our doctors use a combination of history taking, endoscopic examination and skin prick allergy testing to ensure that we arrive at the correct diagnosis and can therefore recommend the most appropriate and effective treatments.
Skin Prick Allergy Testing
Skin prick testing is the gold standard in allergy testing. It is used to confirm which type of pollen is causing the Hay Fever symptoms while also excluding other common nasal allergies such as house dust mite, mould and animal dander.
Nasal Endoscopic Examination
This is a painless procedure used to examine the tissues inside the nose. It is carried out by our doctors during your consultation to ensure there are no structural issues or polyps present within the nose.
Hay Fever Prevention: Pollen Avoidance Measures
Try to
- Keep windows closed during peak pollen hours.
- especially the bedroom window.
- this includes while driving!
- Wear wrap-around sunglasses to help block pollen from entering the eyes.
- Wear a face mask if you plan to cut the grass.... or ask a friend!
- Place Vaseline inside each nostril to prevent pollen from entering the nose.
- Shower and change your clothes after walking in the park.
- Wash bedsheets regularly and vacuum the floors.
- Spend leisure time or holidays at the sea as the sea breeze disperses pollen.
- Check for the next day’s pollen count and plan your schedule accordingly.
Avoid
- Walking in parks and grasslands during pollen season.
- Being outdoors during peak pollen hours (late morning and late afternoon).
- Smoking as this aggravates allergic symptoms and may even contribute to the development of nasal polyps.
- Drying clothes and bedsheets outside as pollen will settle all over your clothes.
Hay Fever Treatments
There are a wide variety of very effective pharmacological treatment options available for Hay Fever. These should be used in conjunction with the avoidance measures detailed above as limiting your exposure to pollen is always beneficial for sufferers.
Oral Medication for Hay Fever
-
Antihistamines: In terms of over the counter medications, non-sedating oral anti-histamines such as cetirizine (Cetrine), loratadine (Clarityn) and fexofenadine (Telfast) can be useful for patients with mild to moderate symptoms. These can be taken on a daily basis during the peak hayfever season or just as required. If anti-histamines result in drowsiness then consider dividing the dose between morning and night or try another brand. Experimenting with different anti-histamines can be useful as some people can find certain anti-histamines either more effective or less sedating than others.
-
Oral decongestants: Pseudoephedrine (Sudafed) can be useful temporarily as a rescue medication.
- Leukotriene receptor antagonists: In cases where asthma or lower airway irritability exists your doctor may prescribe a leukotriene receptor antagonist tablet (montelukast) or steroid inhalers and salbutamol bronchodilators (Ventolin) if this is warranted.
Nasal Sprays for Hay Fever
-
Steroid nasal sprays: These are used when nasal symptoms remain problematic despite the use of anti-histamine tablets. Some brands are available over the counter while others are prescription only. Steroid nasal sprays are considered very safe for seasonal use but they need to be taken every day during the Hay Fever season in order to be effective. Steroid Nasal sprays should ideally be started several weeks before the start of the Hay Fever season.
-
Decongestant Sprays: Xylometazoline (Otrivine, Sudafed Nasal Spray) can be used as a rescue medication but it should be limited to a maximum of 5 days to avoid rebound symptoms and other negative effects.
-
Saline Nasal Irrigation: An effective way to directly cleanse the nasal cavity to reduce mucus, inflammatory mediators and bacterial burden while also improving mucociliary function.
Eye Drops for Hay Fever
- Cromoglicate eye drops such Opticrom are an excellent over the counter option. These work by blocking the 'mast cells' from releasing histamine in the eyes.
- Alternatively, anti-histamine eye drops such as olopatadine (Opatanol) may be prescribed by your doctor.
Advanced Hay Fever Treatment Options
There are two further treatment options for use in more significant cases of Hay Fever.
Allergen Desensitisation Immunotherapy
Immunotherapy is a desensitisation treatment course where a tiny dose of allergen is taken in order to generate immune tolerance and desensitisation to the specific allergy. It is essentially like a vaccination. Immunotherapy is well tolerated and highly effective in those under the age of 40. Significant improvements are expected within the first 12 months.
It is available in both oral and subcutaneous injectable forms but oral tablets are the method of administration primarily used in Ireland. The treatment duration is approximately 3-5 years. At Allergy Ireland, our doctors use sublingual immunotherapy against Grass Pollen, Tree Pollen and House Dust Mite.
Rhinolight Endonasal Phototherapy
Rhinolight provides a highly effective drug free treatment option for nose and sinus allergy sufferers. It is effective in treating the vast majority of cases of nasal Hay Fever symptoms but it does not have any impact on eye symptoms. Rhinolight is used for short, sharp treatments with the benefits lasting for several years.
Hay Fever Treatment during Pregnancy
- It is recommended to cease all medications during pregnancy unless instructed otherwise by your doctor. While none of the medications described above should be used during the first trimester of pregnancy, certain steroid nasal sprays and specific anti-histamines may be used during the second and third trimesters under specialist medical supervision. This should only be done when the benefits outweigh the risks.
- Rhinolight can be used during pregnancy and is highly effective at treating nasal Hay Fever symptoms.
Contact Us to Schedule Your Consultation
If hay fever symptoms impact your quality of life, schedule an appointment for assessment and personalised treatment,
Contact us today to arrange your appointment with one of our specialist allergy doctors.
Hay Fever FAQ's
Does Hay Fever impact Asthma?
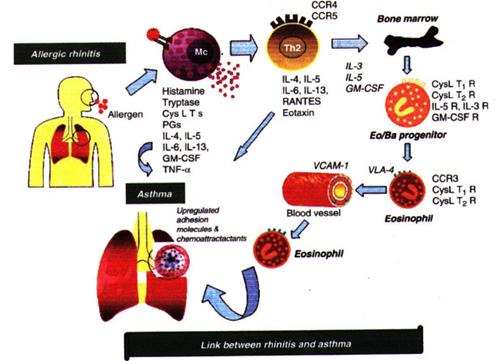
Asthma sufferers with sensitivity to pollen may notice that their asthmatic symptoms can substantially worsen during hayfever season. If the pollen levels are sufficiently high an asthma attack can be triggered in susceptible individuals.
In individuals with Hay Fever, pollen triggers an allergic inflammatory response in all of the mucosal surfaces that it comes into contact with. It is therefore not surprising that pollen which enters the sensitive and reactive airways of asthmatics will irritate and precipitate an allergic response in the lungs just as it does in the nose and eyes.
In addition to pollen directly interacting with the lower airways of the lungs, there is strong clinical evidence that poorly controlled allergic rhinitis itself worsens asthmatic symptoms. In addition, 90% of asthmatics suffer from allergic rhinitis. This makes it particularly important to manage hayfever and rhinitis symptoms in those who have asthma. This 'united airways' approach is now favoured and results in better clinical outcomes for both conditions.
- Hay fever may cause nose symptoms only.
- Hay fever often involves the sinuses as well as the nose.
- Hay fever may provoke chest symptoms.
- Hay fever may go hand-in-hand with asthma.
- Hay fever in asthmatic children is associated with more asthma-related hospital admissions.
Can hay fever develop in adults?
Yes hay fever can occur at any age. Although it is most likely to begin in childhood, sensitisation to pollens can develop in adults who have no history of hay fever.
Why does the Pollen Count vary?
The pollen count is a measure of the amount of pollen in the air over a 24 hour period. Pollen begins to be released early in the morning and is carried by warm air currents high into the air by midday. As the air cools in the late evening the pollen descends again. Cities and concrete urban areas stay warmer for longer and in these areas pollen may even descend during the night. Atmospheric pollution from car fumes and industry can combine with pollen to trigger a more aggressive allergic response. This is sometimes referred to as super pollen by the media.
Do local weather conditions affect Pollen Counts?
Local weather conditions have a significant bearing on the production, dispersal and quantity of pollen grains in the air. Higher pollen counts occur on warm, dry and sunny days. Lower pollen counts occur on wet, damp and cold days. Rain washes the pollen from the air while on shore winds help disperse and remove pollen.
Do different countries have different Hay Fever seasons?
Your own pollen season will vary depending on which pollens you are allergic to and where you live. Certain grass and tree pollens predominate in different countries and the peak release of pollen may occur during different months. Pollen from timothy grass, perennial rye and ragweed circulate throughout Europe in addition to Tree Pollens such as birch which is a common culprit. Some pollens are more common in city environments, forests or mountainous areas. It is worth noting that pollen levels are lower by the sea and that the Grass Pollen season starts about 2 weeks later in mountainous areas.
UK and Ireland
- March - May: Tree Pollen season.
- May - September: Grass Pollen season.
Northern, Central and Eastern Europe
- May - July: Grass Pollen season.
Mediterranean countries
- December – March: Tree Pollen (Birch, Cypress, Juniper, Hazel, Mimosa).
- March – May: Tree Pollens such as American Sycamore.
- April – July: Grass Pollen, Nettle and Olive Tree pollen.
- August – October: second flowering of Nettle and Mugwort Weed.
Why is the prevalence of Hay Fever rising?
The cause for the rising prevalence is unclear but risk factors may include overuse of antibiotics, exposure to air pollution, maternal/passive smoking and climatic factors among other theories.
The Microbiome in early life
Certainly, environmental exposures are key to understanding the rising prevalence of allergies. The ‘hygiene hypotheses’ was proposed as an explanation whereby the more sterile Western lifestyle was reducing infections and resulting in less type 1 immune responses.
More recently, there is a better insight into the development of allergen tolerance with the microbiome during early life being an essential component. Antibiotic use will disrupt this amongst other environmental factors.
Irritants
Exposure to irritants such as cigarette smoke and air pollution, particularly diesel exhaust fumes, have been shown to contribute to and exacerbate Allergic Rhinitis.
Global Warming Extends the Hay Fever Season
In addition, global warming is seen to be playing a role in Ireland with milder weather resulting in prolongation of pollen and spore seasons. This is confounded by the introduction of new pollens such as ragweed which would usually be a common allergen in North America and Continental Europe.
Allergic Rhinitis for Health Professionals
Epidemiology of Allergic Rhinitis
It is estimated that Allergic Rhinitis affects at least 400 million people worldwide and the prevalence within Europe is between 17% and 29%. The UK has a prevalence of 26% and Ireland is likely to be similar to this.
Allergic Rhinitis will often begin early in life but prevalence increases with age. The International Study of Asthma and Allergies in Childhood (ISAAC, 2006) phase III study demonstrated this showing a 5% prevalence in those aged 3 years, an 8.5% prevalence in those aged 6-7 years and a 14.6% prevalence in those aged 13-14 years.
What is most concerning is that the prevalence of Allergic Rhinitis is increasing globally. This was corroborated by this ISAAC study which found an increase in prevalence of Allergic Rhinitis from 13% to 19% over an 8 year period in a cohort of 13-14 year olds. A smaller research study in Cork demonstrated an increase in prevalence from 7.6% to 10.6% over a 5 year period in a cohort of 6-9 year olds.
Detailed Pathophysiology of Allergic Rhinitis
There are two phases which are paramount to the development of an allergy.
Phase one occurs when an atopic individual is first exposed to the allergen. The allergen is taken up by antigen presenting cells, dendritic cells in particular, and processed into peptide fragments. The dendritic cell moves through the lymphatics towards the lymph node where it presents this peptide fragment to a naïve T lymphocyte. The naïve T cell becomes activated to express cytokines such as Interleukin-4 (IL-4) which drives the differentiation of these cells to Th2 helper cells.
An environment rich in cytokines IL-4 and IL-13 is created and is responsible for inducing IgE production from B lymphocytes. Additionally, IL-5 is responsible for eosinophil recruitment and activation. The cytokine profile is vital as it determines a Th2 immune response.
In the meantime, T cell dependent activation of B cells stimulates further cytokine production, particularly IL-4, and promotes irreversible immunoglobulin class switching to allergen specific IgE antibodies.
Allergen specific IgE will attach to mast cells and basophils. This is referred to as primary sensitisation. In addition, memory B cells are generated and a small number of memory T cells remain.
Phase two occurs on subsequent exposure to this allergen. The allergen binds to the sensitised mast cells triggering degranulation of the mast cell releasing pre-stored and newly synthesised inflammatory mediators such as histamine, leukotrienes and prostaglandins. These contribute to vascular permeability, eosinophil infiltration and increased mucus production.
Furthermore, with repetitive allergen exposure nasal priming occurs. This appears to cause an accumulation of effector cells in the nasal mucosa and results in a hyper-responsiveness to the allergen and prolongation of symptoms. In addition, there appears to be a neural component to this hyper-responsiveness. Changes to the sensory nerves of the nose have been demonstrated in those with Allergic Rhinitis. In addition, innate immune responses can be initiated in the nasal epithelium by allergens directly compromising the epithelium and resulting in the release of alarmins such as IL-33 which further potentiates the inflammatory response.
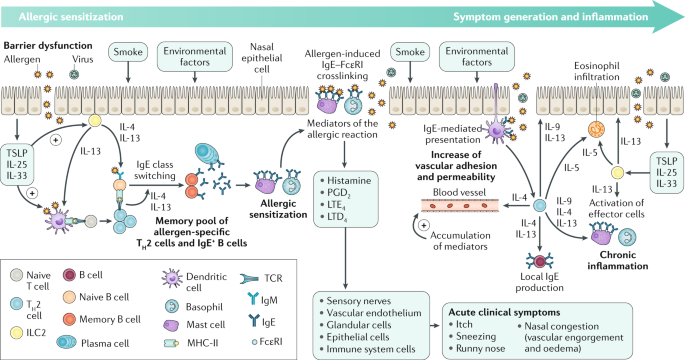
Adapted from Bousquet et al. Nature Reviews Disease Primers, 2020
Allergic Rhinitis Treatment Guidelines for Health Professionals
Non-Pharmacological Management of Allergic Rhinitis
Allergen avoidance should be discussed. Nevertheless, avoidance alone is generally not sufficient to manage symptoms. In cases where the allergen trigger is animal dander avoidance is effective if the animal is removed from the home.
Smoking cessation should be advised always. Smoking can be associated with chronic nasal symptoms and may even be associated with the development of polyposis. Passive smoking or ‘vaping’ appear to carry similar risk.
Saline irrigation of the nasal cavity reduces accumulated mucus, inflammatory mediators and bacterial burden. It has also been shown to improve mucociliary function.
Pharmacological Management of Allergic Rhinitis
In patients with mild intermittent symptoms an antihistamine is often effective. Second generation antihistamines are recommended as they carry less cholinergic and sedating side effects. This includes cetirizine, levocetirizine, loratadine, desloratadine, fexofenadine and bilastine. Oral or nasal decongestants such can be used as a rescue medication but for no longer than 5 days to avoid rebound symptoms.
The ARIA guidelines recommend intranasal corticosteroids as the first line treatment for moderate-severe intermittent or persistent Allergic Rhinitis. A low bioavailability is recommended and so newer generation intranasal corticosteroids are preferred. This includes mometasone furoate (Nasonex), fluticasone furoate (Avamy's) and fluticasone propionate (Flixonase) nasal sprays. Should this not be effective a combination intranasal treatment is now available combining corticosteroid and antihistamine. This includes fluticasone propionate/azelastine hydrochloride (Dymista) and mometasone furoate/olapatadine (Ryaltris) nasal sprays.
If the nasal cavity is very obstructed a nasal spray may not be effective until the oedema has been reduced using intranasal corticosteroid drops such as betamethasone (Betnesol) drops.
Eye symptoms can be managed conservatively with cold compresses and tear supplements. However, if these symptoms persist, it is advisable to consider oral and topical antihistamines, topical mast cell stabilizers (sodium cromoglicate) or decongestants. Topical corticosteroids should ideally be prescribed under the care of an Ophthalmologist.
If there is evidence of lower airway irritability or asthma, a leukotriene receptor antagonist such as montelukast (Singulair) can be trialled. In severe cases short courses of oral corticosteroids are occasionally required.
Additional Treatment Options for Allergic Rhinitis
Immunotherapy
Immunotherapy has been shown to significantly reduce symptoms and medication requirements and is recommended by the ARIA guideline. Additionally, the GINA (Global Initiative for Asthma) guidelines 2022 recommend immunotherapy be considered for asthmatics sensitised to dust mite. Immunotherapy involves exposing a patient to minute quantities of the allergen trigger allowing the immune system to build up a tolerance. It can be given as a subcutaneous injection or as a sublingual tablet. Sublingual therapy is used predominantly in Ireland and is currently available for grass pollen, dust mite and tree pollen. Compliance is crucial and regular follow up advised. It is usually a three year process whereby the patient takes it daily. It is highly effective and well tolerated.
Endonasal Phototherapy
Phototherapy is well established for skin conditions and is now being used within the nasal cavity to manage Allergic Rhinitis. It uses UV-A (25%), UV-B (< 5%) and visible light (70%) to induce a local immunosuppressive effect by inhibiting allergen induced histamine release from mast cells and inducing apoptosis of T lymphocytes and Eosinophils. It essentially desensitises the nasal cavity thus reducing symptoms. It is particularly useful when pharmacological treatment is insufficient or contraindicated.
Does Allergic Rhinitis co-exist with other atopic conditions?
Multimorbid Allergic Rhinitis is where Allergic Rhinitis co-exists with Asthma or Atopic Dermatitis. Interestingly a differing variety of genetically susceptible loci are attributable to multimorbid Allergic Rhinitis, for example IL-5 and IL-33 for those with Allergic Rhinitis and Asthma.
Allergic Rhinitis is a risk factor for asthma. In fact, 90% of asthmatics have Allergic Rhinitis and 30-40% of those with Allergic Rhinitis have Asthma. A ‘united airways’ disease approach to management is the more favoured approach in recent years. Moreover, the treatment of nasal inflammation in asthmatics has been shown to improve outcomes. This highlights the importance of assessing for both asthma and rhinitis in these patients.
Allergic Rhinitis can also be associated with comorbid dermatological conditions such as atopic dermatitis and urticaria upon exposure to an allergen. Interestingly, the treatment of Allergic Rhinitis often results in improvements in these dermatological conditions.